Eyelid surgery Blepharoplasty
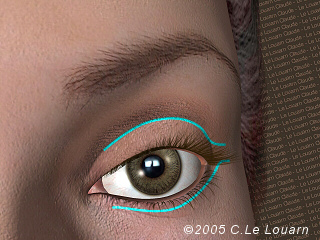
The aim of eyelid surgery is to either rejuvenate the appearance of the eye by treating signs of ageing, or to embellish an eye by changing one or more aspects that are not aesthetically pleasing to the patient, or a combination of the two.
For aesthetic reasons, the patient might want more almond-shaped eyes, a correction of ptosis (the drooping of one of the upper eyelids), or the correction of hereditary hollows under the eyes that manifest themselves from a young age.
As we age, eyelids sag, pouches appear, and hollows become more defined not only below the eye, but also towards the nose and the upper eyelid and the lion’s wrinkle becomes marked. Most patients complain of looking sad or tired. During surgery, excess skin and fat on the eyelids are worked on, as are the hollows below the eyes brought on by age, lion’s wrinkle, the drooping of the corner of the eye, dropping of the cheek bones and to some extent the nasogenian crease.
Different types of eyelid surgery
Standard eyelid surgery
Only excess skin and fat on the lower or upper eyelids can been worked on during eyelid surgery. With this simple and standard surgery, signs of ageing in the ocular area can be greatly improved. However, in certain cases, it can be seen that the eye has been operated on, since one of the signs of ageing is not fully corrected: the eye looks smoother but often deeper set and sometimes even rounder.
The most up to date and sophisticated techniques enable signs of ageing in the ocular area to be treated more comprehensively. There is the disadvantage, however, of operations taking longer. During more comprehensive surgery, it is possible to treat the lion’s wrinkle, the shape of the eye and the hollows by raising the cheek tissue.
Canthopexy lifts the corners of the eyes

When the outer corner of the eyelid droops due to ageing, heredity or a previous operation on the lower eyelids, canthopexy can be performed to reposition the outer angle of the eye. This surgery can be performed on its own (for aesthetic purposes) or carried out during a more in-depth operation to rejuvenate the eyelid.
Treatment of hollow ocular appearance using lipostructure (fat transfer)
It is possible to treat eye hollows with blepharoplasty by taking fat from elsewhere on the body. The fat enables a more definitive action to be taken than when hyaluronic acid, which can be injected at a doctor’s office, is used. The procedure of fat transfer is, however, more complicated. Furthermore, the transfer may not be completely effective and a second operation may prove necessary to further fill the hollow.
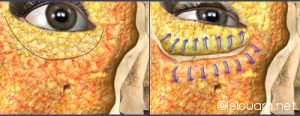
Concentric malar lift: a veritable mid-face lift through an incision in the lower eyelid
The Concentric Malar Lift* is a recently developed surgical technique for facial rejuvenation. It allows the original mid-face structures to be restored, resulting in a harmonious rejuvenation of the gaze using solely a classic incision of the lower eyelid surgery.

As demonstrated in the Face Recurve® Concept, over time, and with repeated eyes’ contractions (blinking, frowning..), the recurrent contraction of a specific segment of the malar portion of the orbicularis oculi muscle and, more particularly, its upper part, pushes the fat tissues located between this muscle and the bone against the orbital bone leading the fat to be expelled toward the surface thus causing a hollowing of the ring at rest : creating a semi-circle crease under the eye: the tear trough as well as two pockets of fat on each side of it the eyelid bags upward and the malar bags downward.
In addition, near the nose, the expelled fat movement down /outward is halted by mimicking a smile expression that has an upwards inverse wave motion. This enhances the nasogenian upper fold.


Leaving a scar flush to the eyelash line of the lower eyelids (same as that made during classic lower eyelid operations), the Concentric Malar Lift
acts like a traditional lower eyelid surgery by:
- removing the lower eyelids excess of skin
- and removing excess of fat out of bags under the eyes,
but also enables to:
- reascend the infra palpebral line under the eyelid (this discrete crease located on a young subject just underneath the inferior eyelid may even be recreate is desired) ,if to achieve a younger appearance by respecting the natural anatomy of the ocular area,
- treat the hollow of the eyes especially in the tear troughs,
- take care of the malar pad thanks to a slight heightening of the cheekbones,
- reduces the upper part of naso-labial fold.
It lifts up the volumes concentrically towards the orbit, to their original position and not upwards or outwardly, whence they do not originate (contrary to “vertical” malar lift).
The global concentric ascent of the tissues allows removing quite more excess of lower eyelid skin (1 to 2 cm), than in the standard lower eyelid surgery (1 to 2 mm), thus increasing the result.
This effect can be used in certain cases in order to cure the result of too ambitious removal of skin during standard technique procedure. The concentric global ascension of the tissues enables here to liberate much needed skin.
One of the aim of the surgery is to tone down the darkness of the mid-face, keeping solely those of the discreet crease under the eyelid, just as women do intuitively when they apply make-up.
The Concentric Malar Lift can be performed :
- on an outpatient basis (neurolept analgesia and a few hours’ stay at the clinic) on its own or together with a surgery of the upper eyelids and, in some cases, without hospitalisation concurrently with a limited Face Recurve® surgery of the lower part of the face (localized specific treatments of the naso labial fold (scar-less/LAN), the bitterness folds and the jowls (scar-less/DAO), and the cervical bands (discreet sub mental scar)
- with hospitalisation at the same time than a classic facelift surgery(neck, cheeks, temples…) or a Face Recurve® Lift (classic Face Lift + specific treatments Face Recurve® of the naso-labial fold , the bitterness folds , the jowls and the cervical bands).
Warnings and therapeutic alternatives to eyelid surgery
Blepharoplasties do not treat pre-existing asymmetries (ptosis, corners of the eyes…) unless treatment targets them specifically. However, like after any aesthetic operation, it is usual for the patient to look at and analyse themselves more, and, since the features that they did not like have been treated, certain patients come not to like a pre-existing asymmetry that they had seen as insignificant prior to the operation. Therefore, it can be useful to discuss possible corrections of asymmetry prior to the operation.
Whatever the surgical technique used, the result can usually be accentuated by :
1. filling injections – hyaluronic acid (immediate results but an absorbable product, thus requiring further injections)
2. botulinum toxin injections* to smooth out crows’ feet, to raise eyebrows, to act on the lion’s wrinkle, to make eyes look larger, etc. a film on botulinum toxin is available
3. techniques used on the epidermis such as flash lamps, lasers and peeling. Ageing brought on by exposure to the sun manifests itself by wrinkles, a crumpled look and blotches. Good results can be achieved on these by using skin abrasion techniques: peeling, laser or pulse lamps. Eyelid surgery is not particularly effective on the appearance of the epidermis.
Dark circles can be due either to an over pigmentation of the skin, to a depression that casts a shadow or to both factors in tandem. Skin colouration can very often be treated by the chemical action of a pigmentation creams or peeling. These techniques aiming at “making new skin” are satisfactory if there is limited exposure to the sun afterwards and if the risk of pigmentation problems are correctly assessed in function of the type and state of the skin.
NB: Dr Le Louarn prefers to refer you to a dermatologist for techniques that specifically tackle the epidermis (flash lamps, lasers, peeling etc.)
In some cases, it may even be required to add one of the above mentioned techniques to surgery in order to obtain the desired effect.
It should be noted that these techniques (dermal filler, botulinum toxin or epidermis abrasion) can also be carried out on younger patients to delay the operation by combating symptoms from the outset, or with more limited results on more marked patients not wishing to undergo an operation.
To treat hollows, a filling product (fat or hyaluronic acid) can be carefully injected, but when there is a clear excess of skin, only a malar lift of the cheek tissue will give a satisfactory result.
Operations
Practical recommendations prior to the operation
In the case of ocular pathology, the consent from your ophthalmologist is required before embarking on an operation. The surgeon could alternatively ask you to undergo a pre-op ophthalmologic assessment.
Do not arrive too morally or physically tired to the operation. Let us know about any change in your state of physical or mental health and do not forget that there is never any urgency to carry out an aesthetic operation.
Medicines that cause bleeding are prohibited during the days leading up to the operation: Aspirin, Anticoagulants…. …
It is imperative that all aesthetic operations be foregone if you are ill or, for women, if you are pregnant on the day of the operation. You must not drink or eat during the 6 hours prior to the operation.
The operation will be cancelled if preoperative advices are not adhered to.
When preparing your belongings, DO NOT FORGET YOUR MEDICAL FILE.
Where possible, do not bring any valuable jewellery with you (or put it in the safe at the clinic with your other valuables during the operation.)
Have a shower or bath before coming to the clinic and wash your hair; women should obviously not wear nail varnish or make-up. Wear comfortable clothing when you come to the clinic.
It is imperative that contact lenses, dentures and hearing aids be removed before you are given an anaesthetic. If you wear contact lenses you will not be able to use them for 5 – 10 days after the operation, so make sure you have a pair of glasses ready.
Anaesthetic and hospitalisation
Usually these operations do not require the patient to stay in hospital and are performed in ambulatory under neuroleptic analgesia (assisted local anaesthetic). The patient is usually discharged a few hours after the operation. However, in certain cases (nausea, stress etc.) it is preferable for the patient to stay in hospital overnight.
Sometimes, if the operation is limited, a local anaesthetic can be administered in the presence of an anaesthetist.
Going home after the operation
Ask an ABLE-BODIED AND RESPONSIBLE person to take you home since anaesthetics are euphoriants and your vision could be blurred during the hours after the operation.
Do not make any plans to do anything requiring concentration or the use of potentially dangerous equipment. If you are going home by car YOU WILL NOT BE ABLE TO DRIVE UNDER ANY CIRCUMSTANCES. Bring a pair of sunglasses with you if you want to leave the clinic more discreetly, but do not let go of the arm of the person accompanying you.
At home
Before leaving home prior to the operation, make sure that you prepare everything for when you return:
– Prepare a light meal
– Put Arnica 5CH, paracetamol-based painkillers (Dafalgan, Doliprane) a bottle of mineral water and your ointment on your bedside table.
Arrange for someone to be with you at home. You should not get up during the night following the operation without being accompanied even to go to the toilet and even if you feel perfectly fine (anaesthetics can cause effects identical to those of alcohol abuse.)
The next steps
In theory, no pain but discomfort will be experienced with some watering of the eyes during the first days after the operation and, in exceptional cases, problems of vision immediately after the operation.
You should initially relax as much as possible and avoid any over exertion. However, you should walk a bit every day to prevent the risk of embolisms and eat enough to help with the healing process.
Bruises usually remain for 6 to 20 days and can be concealed with make-up once stitches are removed.
Swelling is at its worst on the 3rd to 4th day after the operation and then fades progressively. In addition to common products such as Arnica or Auriderm, cold compresses calm bruises and swelling, helping them to heal more quickly. The face can also be drained by temporarily adopting a sleeping position with the chest slightly raised.
For 1 to 2 months there may be a limited hardening at the outer corner of the eyes. This is temporary and is usually not visible by others.
You will probably need to wait:
– 7 days before being presentable enough for those close to you to see you and for you to be able to go out in public without getting strange looks
– 12/15 days before meeting up with friends…and going back to work
– 3 weeks to 1 month before meeting up with people close to you who you do not want to know about the operation.
The consequences differ depending on the reactions of each individual and the sophistication of the operation performed. For example, people with a strong pigmentation under the eyes will have persistent bruising on the lower eyelids. Swelling and potential hardening are variable on each side and an asymmetry sometimes is apparent after the operation, yet this does not have any negative effects on the final result.
Leave from work: 1 to 2 weeks depending on your profession
Stitches removed after 3 to 6 days
Bruises for 6 to 20 days
Swelling very visible for 15 days
Note down the telephone number of the surgery, (01 45 53 27 17 from France and 33 1 45 53 27 17 for international call), and the number of the clinic near your home telephone and in your mobile phone. Do not hesitate to call us if you are worried. Call us if you have a temperature, experience weeping, pain or other symptoms that give you cause to worry.
Risks
In most cases operations go smoothly and patients are satisfied with the results. However, before deciding to undergo an operation, you should be aware of all risks of resulting imperfections and of possible complications.
General risks of all surgical operations: infections, haematomas, healing problems and risks from anaesthetics
Infections
If an operation is performed under normal conditions and post-op care and advice are adhered to, infections are very seldom. You will be notably asked to respect cleanliness guidelines and to apply ointment to prevent conjunctivitis.
Haematomas
The risk of haematomas rises considerably when medicines that can cause bleeding are taken pre and post-op.
Haematomas are usually not serious and can be halted when they are significant. However, during the hours following the operation, if strong pain from the eyeball pushing outwards is experienced, it could be the result of a retro-orbital haematoma (a haematoma behind the eye that pushes the eyeball forward.) This complication requires urgent treatment to avoid deterioration into blindness (a fully exceptional risk but nevertheless reported in international scientific publications.)
Healing problems
The appearance of small epidermal cysts on scars does not in any way compromise the quality of the final result. If the cysts do not disappear on their own, they can be easily treated by the surgeon during a follow-up session with the patient.
Very occasionally scars may need to be treated after the first operation to correct scar expansion.
Risks from anaesthetics
Anaesthetic techniques and monitoring methods have improved immensely and safety is high when an operation is performed in non-emergency conditions on a person in good health, when the anaesthetist is competent and working in a recognised establishment. However, the effect of anaesthetics on the body can be difficult to predict and treat. Therefore there are still risks and hazards inherent to all anaesthetics before and after the operation. This is why it is imperative that you consult the anaesthetist prior to the operation and fully inform him of the state of your health. In function of your health and the planned operation, he will assess the risks related to anaesthetics and tell you of any potential precautions to take. If the anaesthetist objects to the operation, this decision is final.
(see in chapter ” Before surgery ” section “Check up and anaesthetic consultation“)
Risks during any aesthetic operation: asymmetry, a result judged as insufficient or excessive, need to touch up results, sensitivity issues
The way in which tissues react to an operation is always specific and, to a certain extent, unpredictable. It depends on the patient correctly following the doctor’s recommendations, but luck also plays a role. This is why all risks of asymmetry, unsatisfactory or excessive results and the need to touch up results are evoked prior to any aesthetic operation.
Issue for eyelid surgery:
Imperfections of the result
Certain problems once results can be seen come from misunderstandings between the patient and the surgeon concerning the aim of the operation or decisions taken without due consideration. This risk can be limited by carefully thinking the procedure through well in advance.
Other problems arise from unexpected tissue reactions specific to the patient that can lead to an excessive, insufficient or asymmetric result. This risk principally concerns patients with a poor quality of skin, but retractile fibroses are always possible. If resulting imperfections are difficult to bear, they could potentially be surgically touched up later – an operation that is much less intense than the first. However, it is necessary to be patient and to wait until the healing cycle comes to an end before embarking on a second operation.
Sensitivity
When hollows are treated by lifting the cheekbones (concentric malar lift) paraesthesia (uncomfortable temporary sensations) can occur on the top lip.
Specific eyelid surgery risks:
Sunken eye
If too much fat is removed when standard techniques are used, the eye can appear too sunken.
Upper eyelids
If an excess of skin is removed, it can initially be difficult to close the eye completely (lagophtalmia).
Lower eyelids
The eye can become rounder or even show an eversion. This type of problem is always temporary when resulting from considerable scar retraction pulling the eyelid downwards. When the problem stems from the quantity of skin removed, it is always possible to touch it up afterwards in a later session.
Functional problems
Exceptional cases of diplopy (double vision) and glaucoma (ocular hypertension) have been reported.
The result
An initial evaluation of the final result can be made two to three months after the operation. However, the scars and tissues may still be inflamed at that time which is why, in order to judge the definitive result, it is best to wait for six to nine months after the operation. Most often an appreciable rejuvenation effect is achieved giving a relaxed and refreshed appearance, often coupled with a better psychological state.
Secondary ageing could be reduced by using botulinum toxin injections to limit facial ageing caused by movements and by limiting exposure to the sun.
By way of conclusion, we remind you that precise and detailed information, an in-depth analysis of the reasons for the operation, teamwork between the patient and the surgeon during the preparatory phase, the search for surgical excellence coupled with a good analysis of benefits and risks, the respect of pre-op and post-op advice and regular monitoring of the patient are all key elements for aesthetic surgery to be a success.
References
Some information about blepharoplasties is available in English on the page « Eyelid surgery» of ISAPS’website (International Society of Aesthetic plastic Surgery), chapter: « Info for patients ».
www.isaps.org
Some information is also available in French on the page « Blepharoplasty » of the SOFCPRE’s website (Société Française de Chirurgie Plastique Reconstructrice et Esthétique) : www.plasticiens.org
Specific information deliverd on this website is based on Doctor Le Louarn’s practice and on his scientific works:
1 – LE LOUARN C, BUTHIAU D, BUIS J. : Structural aging: the Facial Recurve concept
Aesthetic Plast Surg. 2007 May-Jun;31(3):213-8.
http://www.ncbi.nlm.nih.gov/pubmed/173803582 – LE LOUARN C, BUTHIAU D, BUIS J. : The Face Recurve concept: medical and surgical applications
Aesthetic Plast Surg. 2007 May-Jun;31(3):219-31; discussion 232.
http://www.ncbi.nlm.nih.gov/pubmed/174840583 – LE LOUARN C, BUTHIAU D, BUIS J. : Rajeunissement facial et lifting malaire concentrique: le concept du FACE RECURVE®
Facial rejuvenation and concentric malar lift: the FACE RECURVE concept
Ann Chir Plast Esthet. 2006 Apr;51(2):99-121.
http://dx.doi.org/10.1016/j.anplas.2005.12.016
http://www.ncbi.nlm.nih.gov/pubmed/165303164 – LE LOUARN C. : The Concentric Malar Lift and lower eyelid rejuvenation
Aesthetic Plast Surg. 2004 Nov-Dec; 28(6):359-72;
http://www.ncbi.nlm.nih.gov/pubmed/156453385 – LE LOUARN C. : Chirurgie Esthétique faciale par la voie d’abord palpébrale supérieure
Aesthetic facial surgery through the upper blepharoplasty incision
JFORL vol 45/numero 4/1996
http://cat.inist.fr/?aModele=afficheN&cpsidt=32408626 – LE LOUARN C., CORNETTE DE SAINT CYR B. : Incision Cutanée dans le Lifting Lambeau de SMAS Cervico-Malaire Oblique et Lifting Malaire
Cutaneous incision in facelift. Oblique cervicomalar SMAS flap and malar facelift.
Ann Chir Plast Esthet. 1994 Dec;39(6):756-64. French.
http://www.ncbi.nlm.nih.gov/pubmed/76615597 – LE LOUARN C. : Surgical treatment of the rings around the eyes – Elsevier
Plastic Surgery 1992 . Vol II. U.T. Hinderer, editor8 – LE LOUARN C. : The malar S.M.A.S. flap – Elsevier
Plastic Surgery 1992 . Vol II. U.T. Hinderer, editor :517-89 – LE LOUARN C. : Traitement Chirurgical des Cernes – Surgical treatment of rings around the eyes
Ann Chir Plast Esthet. 1989 ; 34(6):513-6.
Cet article a été selectionné et publié par le « Year Book of Plastic and Reconstructive Surgery »
Mosby, 1991 : Surgical treatment of the rings around the eyes
http://www.ncbi.nlm.nih.gov/pubmed/248269410 – LE LOUARN C. : Le Lambeau Musculo-Graisseux Malaire = The malar SMAS flap
Ann Chir Plast Esthet. 1989; 34(6): 510-2.
http://cat.inist.fr/?aModele=afficheN&cpsidt=6680022
The following publications and works can also be listed ( this list is obviously not exhaustive and may be amended) :
1 – LITTLE J.W. : Structural aging: the facial recurve concept
Aesthetic Plast Surg. 2007 Nov-Dec ; 31(6):754-6.
http://www.ncbi.nlm.nih.gov/pubmed/179851772 – MENDELSON B.C., HARTLEY W., SCOTT M, McNAB A., GRANZOW J.W. : Age-related changes of the orbit and midcheek and the implications for facial rejuvenation
Aesthetic Plast Surg. 2007 Sep-Oct ; 31(5):419-23
http://www.ncbi.nlm.nih.gov/pubmed/174864023 – CORNETTE DE ST CYR B., GAREY L.J., MAILLARD G.F., AHARONI C. : The vertical midface lift. An improved procedure
J Plast Reconstr Aesthet Surg. 2007; 60(12):1277-86
http://www.ncbi.nlm.nih.gov/pubmed/175696064 – HAMRA S.T. : The role of the septal reset in creating a youthful eyelid-cheek complex in facial rejuvenation
Plast Reconstr Surg. 2004 Jun; 113(7):2124-41
http://www.ncbi.nlm.nih.gov/pubmed/152532085 – FOGLI A.L. : Orbicularis muscleplasty and face lift: a better orbital contour.
Plast Reconstr Surg. 1995 Dec ; 96(7):1560-70
http://www.ncbi.nlm.nih.gov/pubmed/74802766 – FLOWERS R.S., FLOWERS S.S. : precision planning in blepharoplasty. The importance of preoperative mapping
Clin Plast Surg. 1993 Apr; 20(2):303-10
http://www.ncbi.nlm.nih.gov/pubmed/84859407 – JELK G.W., JELK E.B. : Repair of lower lid deformities
Clin Plast Surg. 1993 Apr ; 20(2):417-25
http://www.ncbi.nlm.nih.gov/pubmed/84859508 – HAMRA S.T. : Repositioning the orbicularis oculi muscle in the composite rhytidectomy
Plast Reconstr Surg. 1992 Jul;90(1):14-22
http://www.ncbi.nlm.nih.gov/pubmed/16150819 – JELK G.W., JELK E.B. : Blepharoplasty – Chapter 5 in Complications and Problems in Aesthetic Plastic Surgery
Edited by George C. PECK – Gower Medical Publishing 1992 : ISBN 0-397-44613-610 – ADENIS J.P. , MORAX S. Chirurgie palpébrale
Doins éditeurs Paris 1992 – ISBN 2-7040-0647-411 – MORAX S., PASCAL D., BARRACO P. : Traitement chirurgical des ptosis par désinsertion de l’aponévrose du releveur de la paupière supérieure
Surgical treatment of ptosis by the disinsertion of the aponeurosis of the elevator muscle of the upper lid
Bull Soc Ophtalmol Fr. 1985 Nov;85(11):1145-8.
http://www.ncbi.nlm.nih.gov/pubmed/384317712 – REES T.D. : Blepharoplasty
Part 3 in Aesthetic Plastic Surgery, Volume I
Edited by Thomas D. REES – Saunders 1980 : ISBN 0-7216-7519-013 – ROUGIER J., TESSIER P. et coll. : Chirurgie esthétique des paupières
chapitre 26 dans Chirurgie plastique orbito-palpébrale
Rapport de la Société Française d’Ophtalmologie – Masson, Paris 197714 – TESSIER, P. ROUGIER J., and coll. : Ouvrage traduit par WOLFES S.A. Esthetic surgery of the eyelids
Chapter 26 in Plastic Surgery of the orbit and the eyelids
Masson Publishing USA 1981 : ISBN 0-89352-041-1