Surgical rejuvenation of the face: facelift, face recurve® & face recurve® lift
Theories and principles of surgical rejuvenation
Facial ageing depends on several factors: heredity, health behaviour (sleep, sun exposure, cigarettes), state of health (medical and psychological : negative effect of stress), and also greatly on weight stability.
Historically, the facelift was initially developed to treat the effects of age by dealing with the problem of excess skin: this is the traditional facelift that “lifts”, i.e. pulls and makes the skin taut. The problem with this technique is that the result it generates is often inconsistent, as only the surface is treated. If the sought-after effect is important, the danger is that the result might be “very unnatural”: as if a wrinkle-free mask had been placed on an ageing and sagging structure.
Subsequently, with the evolution of surgical techniques and thanks to the works initiated by Dr Paul Tessier, it became possible to deal not only with the problem of excess skin but also with the overall sagging (or the ptosis) of the face.
On the upper part of the face, sub-periosteal lifts are performed: mask-lift and vertical lifts which are meant to bring the tissues of the upper face upwards and backwards . The result of these procedures is much more satisfactory aesthetically and much more stable over time than the simple traction of conventional lifts since their sub-periosteal action provides in-depth treatment, while the surface is treated by excision of the excess skin.
Vertical lifts bring the cheekbones and the temples upwards and backwards; mask-lifts additionally lift the forehead. As these two procedures modify the features, namely by brightening up the gaze, they often allow achieving not only a more youthful face but also an embellishment thereof. The main drawback for the patient is the logical consequence that follows, i.e., the necessity to cope with the reaction of the people around because of the changed gaze.
On the lower part of the face (neck, oval and cheeks), the facelift is presently treated via a muscular approach additionally to treated the skin problem, thereby achieving greater, more stable traction .
Such facelifts may be considered as of the first signs of ageing (usually starting from 40/45 years), or if the patient is motivated and a frank psychological benefit is expected from the operation. In the particular case of the Mask-Lift, this may be considered even earlier (20/25 years of age) with the intent of improving the facial features (see below).
When all is said, periosteal and muscular lifts have provided for really improving rejuvenation surgery results. However, it is to be noted that their efficacy in terms of paramedian structural ageing repair (folds between the eyebrows, caved in rings under the eyes, naso-labial folds, bitterness folds, and cervical bands) can prove limited.
Advanced Face Recurve® protocols include surgical rejuvenation. Besides treating excess skin and ptosis, surgery is now capable of improving the paramedian folds, as well as preventing secondary structural ageing.
Face Recurve® : a new philosophy in structural ageing
The Face Recurve® concept is the fruit of recent studies (C. Le Louarn, D. Buthiau, J. Buis) on structural ageing that has made it possible to come up with a new analysis of this ageing process and with new medical and surgical treatments for each ageing stage and, finally, to develop a new specific anti-age strategy dealing with structural ageing.
Face Recurve® offers simultaneously:
– a new rationale for structural ageing,
– new surgical and medical treatments in the fight against this ageing process,
– and a new specific anti-age strategy to deal with structural ageing.
EXPLANATION
The overall ageing process may be broken down into two types of differing rationale and which do not, therefore, respond to the same treatments, i.e., cutaneous ageing and structural ageing.
Cutaneous ageing has to do with age-related tegument alteration, i.e., the skin. This is manifested by loss of elasticity (the creased and thinned-out look), discolorations (pigment spots), blotches, dilated pored.
Structural ageing involves the deep structures, i.e., bones, fat tissues and muscles). This is manifested by the occurrence of hollowed paramedian furrows (places symmetrically on each side of the face): rings under the eyes, naso-labial folds, bitterness folds, cervical bands, as well as the occurrence of excess tissue volumes (bags under the eyes, jowls…) and, later, sagging of the face.
Gravity had long been thought to be responsible for structural ageing, that is, the sagging of the face with excess skin was imputed to it.
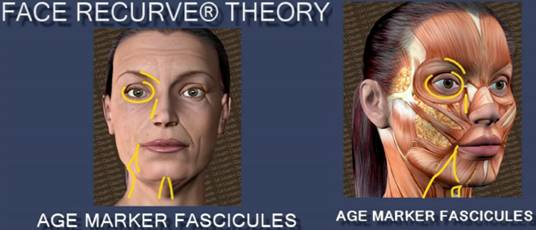
Scientific studies (clinical, anatomic and radiological) conducted by the Le Louarn-Buthiau-Buis team have evidenced that structural ageing of the face is primarily of muscular origin, and that is especially induced by expression muscle fascicles or age marker fascicles (AMF).
With time and repeated contractions, the expression muscles change from curvilinear and long in young subjects to rectilinear and contracted in the elderly. The mechanism causes the formation of paramedian furrows and fat mass volumes.
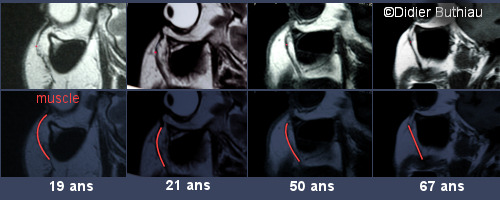
Photos taken by radiologist Doctor Didier Buthiau during an IRM study to confirm the Face Recurve® theory.
In the pre-malar area of two normal body-weight subjects aged 19 (left) and 67 (right),
there is apparent loss of muscle curvature and reduced deep fat tissue volume compensated for by superficial fat.
This mechanism is greatly amplified by specific expression muscle segments called Age Marker Fascicles (AMF).
This system proves particularly effective as an indicator of the individual’s biological status because the tissue masses formed from the ejected fat localize along the folds parallel to the marker fascicle involved. For example, the fat volume found above the naso-labial fold enhances the visibility of the corresponding furrow and vice versa.
Gravity only comes in secondarily once the tissues are already damaged by the marker fascicle action and the skin ageing process.
As Face Recurve® has allowed for a new understanding of the ageing process, a number of medical techniques specifically intended for countering the AMF deleterious action have developed , the goal of all these techniques being to preserve or restore the anatomic structure as closely as possible to that of the young subject.
This is achieved through:
– blocking the action of the age marker fascicles (AMF impairment by Botulinum toxin or specifically targeted surgical AMF section);
– the camouflage (using fillers) or correction of the fat volume losses (by surgically returning the fat tissue to its initial place).
For example, to date the jowl was treated during the facelift by pulling the skin as much as possible upwards towards the ear. However, cutaneous traction alone could not resist the repeated action of the mimic muscle which pulls the jowl downwards (pouting). Now, thanks to an appropriate sectioning of the marker fascicle responsible for the jowl (DAO) and the replacement of the fatty volumes expelled by the contraction of the DAO, the facelift is only required for the resection of the excess skin. The result on the jowl is more effective, natural and stable.
Face Recurve® has therefore, for the first time, made it possible to treat both the consequences (excess skin and sagging) and their cause (age marker fascicles). In particular, the traction of the facelift or the filling are no longer called upon to delete the after-effects of the action of the expression muscles . The excess skin is removed and the volumes are replaced in strict observance of their initial positions and volumes. We thus avoid the pulled appearance (skin pulled too tautly in order to achieve the required effect on a median furrow lying at some distance from the scar) or a puffy appearance (excessive filling to hide the furrows and absorb the excess skin). The anatomic structure is thus restored to resemble that of the young subject and the resection makes it possible to curb the damaging action of the marker fascicles and therefore to prevent subsequent structural ageing.
The drastic change induced by Face Recurve® in the analysis of the structural ageing mechanism has finally led one not only to the introduction of new medical and surgical techniques, but also to the development a real strategy in the struggle against structural ageing.
For further details on Face Recurve® please, refer to the article under same heading. See also the 3 D video showing the visibility of the process. Link to “Face Recurve®” article.
The various facial rejuvenation surgical techniques
Localised Face Recurve® surgery
In the treatment of structural ageing Face Recurve® offers an intermediate solution between cosmetic medicine (Botulinum toxin and fillers) and the facelift. This is a local surgical procedure aimed at correcting the marker fascicle shortening and the induced fat tissue displacement.
Localised Face Recurve® Surgery
Age marker fasicles sections
The Face Recurve® surgical procedure is proposed as a sole treatment when local repair of the structural ageing involving the median area is desired (rings under the eyes, naso-labial folds, jowls, bitterness folds, cervical bands) and when a facelift is not justified, i.e., if the excess skin problem has not set in, the face is marked by the skin has retained tonus. Targeted Face Recurve® surgery is also indicated supplementary to a standard facelift, when results on paramedian ageing features are inadequate.
The procedure is done on an outpatient basis, either using local anaesthetics or under assisted local anaesthesia , depending on the number of areas treated.
Using a limited incision, the surgeon cuts one or several age marker fascicles and places back to its original position the fat tissue that has been ejected due to the AMF action over time. The expression muscle convexity is thus restored. The patient looks structurally younger and his/her anatomic features match those his/she had initially to the utmost.
A well-targeted injection of Botulinum toxin is administered during the operation to ward off the regeneration of the sectioned muscle fascicle. Many sports traumatology studies have been carried out showing that immobilization of injured muscle during the healing phase prevents it from healing. Thanks to the additional action of Botulinum toxin it has become realistic not only to expect to treat structural ageing locally with the Face Recurve® surgery, but at the same time to block subsequent muscle regeneration thereby forestalling the structural ageing process itself.
The Face Recurve® procedure as performed alone does not create any long scars covered up by the hair, since no skin re-draping (facelift) is associated but only localized action is induced. The naso -labial folds are managed by small incisions hid inside the nose, while the jowls and bitterness folds are corrected from within the mouth and cervical bands treatment leaves but a small scar under the chin.
With Face Recurve ® it is now possible to plan:
– to treat the consequences (naso -labial folds bitterness folds and cervical bands ),
– to act on the cause (age marker fascicles),
– and to stabilize the results (the secondary structural ageing process is checked with Botulinum toxin).
Cervico-Facial Lift and Cervico-Facial Face Recurve® Lift
The cervico-facial lift involving the area from neck to temples is the most common type of facelift performed. The aim is to treat the sagging and drooping of the skin and muscles of the face and neck. The operation is intended to restore a younger appearance rather than to change actual features.

Cervico-facial lift.
Either a complete cervico-facial lift (neck, cheeks, and temples) or an oval lift (neck / jowls) can be performed. The cervico-facial lift can be performed either separately or in conjunction with numerous other facial aesthetic procedures such as frontal lifts, blepharoplasty (rejuvenation of eyelids), canthopexy (elevation of the corners of the eyes), concentric malar lift (rejuvenation of the central area of the face/see below), and skin abrasion (peeling, laser treatment, dermabrasion).
When the cervico-facial lift is performed according to conventional techniques, it is less effective on the median zone than on the lateral sides of the face. It therefore has a rather limited and short-term effect on structural ageing: naso-labial folds, bitterness folds and cervical bands.
When a cervico-facial lift is combined with the Face Recurve® involving the paramedian folds, the procedure is referred to as cervico-facial Face Recurve® Lift.
The muscle sectioning and fat tissue transfer specific to Face Recurve® are performed concurrently to a cervico-facial lift during the surgical procedure. The paramedian folds of the operated zone are thus specifically corrected with Face Recurve®, while the cervico-facial lift deals with the excess skin.

Cervico-facial Face Recurve® Lift.
Cervico-facial lift
Blue area = Detachment zone
Blue line = Scar
+ Face Recurve®
In yellow = The age marker fascicles treated during the operation.
In red = The sections of these fascicles.
=> Action on the upper aspect of the naso-labial fold, the bitterness fold, the jowl, the cervical bands.
In pink = Horizontal plication of the PL muscle to treat the sub-maxillary gland.
Thanks to targeted AMF sectioning and fat tissue transfer, the facelift procedure is no longer expected to exert traction to erase the sequels related to the expression muscle action. The facelift is thus restricted to excess skin resection and the risk of obtaining a taut face, which used to result from the use of a conventional technique whereby a neat appearance was sought by pulling too tightly on the skin to act on prominent medial folds far removed from the scar.
The excess skin is cut out and the tissue volumes are put back in place with strict respect of their former location and volume. The anatomic structure is thus restored as closely as possible to that of a younger subject while AMF sectioning provides for controlling their deleterious action, thereby holding back the ongoing skin ageing process. Results are more effective, natural-looking and stable.
The procedure requires one to two nights’ hospital stay. It is carried out under general anaesthesia or assisted local anaesthesia, depending on the case.

Concentric Malar Lift
When eyelid surgery is combined with a Face Recurve® procedure confined to the palpebral region, this is referred to as Concentric Malar Lift.
The Concentric Malar Lift* is a recently-developed surgical technique for facial rejuvenation. It allows the original centre-face structures to be restored, resulting in a harmonious rejuvenation of the area. Leaving a scar flush to the eyelash line of the lower eyelids, the Concentric Malar Lift acts on the lower eyelids, the hollow of the eye, the dark circles around the eyes, the cheekbones and the upper part of naso-labial fold . It lifts up the volumes concentrically towards the orbit, to their original position and not upwards or outwardly, whence they do not originate.
The operation can be carried out either separately on an outpatient basis (neuroleptanaesthesia and a few hours’ stay at the clinic) or concurrently with Face Recurve® of the lower part of the face (scar-less limited action on the bitterness folds, on the jowls and on the cervical bands) or within a Face Recurve® Lift.

Frontal lift
The frontal lift aims at correcting the ageing process in the upper facial area; it can be performed separately or concurrently to other facial cosmetic procedures such as temporal lifts, cervico-facial lifts, blepharoplasty, canthopexy, concentric malar lifts, skin abrasion.
Some surgeons carry it out by endoscopy, whilst others prefer to pass through the upper eyelids.
The scar can be placed under the hair, but the traction moves the hairline backwards so that the forehead can become disproportioned. The risk of the hairline recessing is the same for endoscopic lifts, although the scars under the hair are shorter.
When the forehead is naturally prominent, frontal lifting with a scar flush to the hairline is the only procedure to consider. The disadvantage is, of course, the possibility for the scar to be apparent. The same can be hid after the operation, if necessary, either by a tattoo or by micro-hair transplant.
It should be noted that the development of the Face Recurve® concept has had practically no effect on forehead surgery, as the fatty layer in this area of the face is extremely thin. The only marker fascicle in the forehead area is responsible for the lion’wrinkle (corrugator). Surgical or medical actions on the latter (respectively, by sectioning or by Botulinum toxin injection to limit its contraction), have been commonly used for several years.

A special case: the mask-lift
This is a special lifting technique invented in the 1980s by Dr. Paul Tessier.
The aim of the mask-lift is embellishment rather than rejuvenation. It enlarges the forehead, lifts the eyebrows, creates almond-shaped eyes and raises the cheekbones. It causes a naturally sad face to be brightened up. The technique harmonises a face that is too long and changes faces that are perceived as too masculine into more feminine ones. The scar takes the form of a headband.
The mask lift is performed under general anaesthesia during an overnight hospital stay.
As it modifies the features, it is more suitable for young people than for those who have very well-established and settled lives, as their entourage may find it difficult to accept their change of appearance.
Conclusion
A modern rejuvenation surgery must be adapted to the shape and dynamic of the face but also to the effect desired by the patient. Some patients merely want to look “healthy”, while others want maximum effectiveness. It follows that the surgeon carefully discusses the action that could be taken in each area of the face and the probable results with the patient (e.g.: a moderate or clear effect on the oval of the face, clearly raising the eyebrow in the centre and less markedly on the tail, action merely on the forehead or only on the oval…). Nowadays it is perfectly possible and desirable to carry out “made to measure” facelifts, but it is important not to lose sight of the fact that:
– T reatment of excess skin alone without a correction of the structural ageing of the face can produce a result that will intuitively be seen by others as inconsistent. Notably in the mid-facial area, dark circles will remain, as will a deep naso-labial fold and a drooping mouth, whilst the lateral part of the face will be very taut.
– On certain emaciated faces, re-draping, muscle tightening, Face Recurve® or even a Face Recurve® Lift are not recommended unless accompanied by an adapted filling action, since tightening on a face that has been considerably hollowed by age inevitably accentuates the visibility of underlying fat-tissue waste, thereby creating a “mummified” appearance.
Warnings and therapeutic alternatives
The facelift and/or the Face Recurve® procedures do not treat pre-existing asymmetries unless treatment targets them specifically. However, as is the case after any aesthetic operation, it is usual for the patient to look at and analyse themselves more than before, and, since the features that they did not like have been treated, certain patients come not to like a pre-existing asymmetry that they had seen as insignificant prior to the operation. Therefore, it can be useful to discuss possible corrections of asymmetry prior to the operation.
If re-draping of the skin is desired without resorting to surgery, the Thermage technique is of interest provided one has to do with a “good case”: not too much excess skin and still a good tonicity thereof, in which case Thermage can be effective on the excess skin problem. Using deep electric micro pulses, this process causes a warming up of the dermis without involving the epidermis and causing consecutive tissue retraction. A single treatment session is needed and there are no ensuing social consequences. Nonetheless, it is to be noted that even if the patients are screened, 20% of them remain resistant to the treatment and obtain no results, versus 80% who are improved.
Regardless of the surgical technique used, results can be made more coherent by combining techniques that act on the epidermis, such as Flash lamps, laser therapy, peeling, etc….
– Sun-related skin ageing is manifested by fine wrinkles, a crease-marked appearance, and spots, all of which can be fairly successfully managed by skin abrasion techniques like peeling, laser or pulse lamp treatments, dermabrasion. As for the facelift, it is of very little efficacy as far as the epidermis is concerned. Inasmuch as these techniques are aimed at “make one’s skin new”, they are satisfactory provided sun-exposure is restrained during the post-treatment period and that any skin pigment disorders have been adequately assessed according to the type of skin and condition thereof.
NB: Dr Le Louarn prefers to refer you to a dermatologist for techniques that specifically tackle the epidermis (flash lamps, laser, peeling etc.), as well as for Thermage treatments.
In many cases, the surgical results may be enhanced by added local cosmetic treatments on the non-treated areas, namely:
– Filling injections with hyaluronic acid (immediate results but this is an absorbable product requiring further injections);
– Botulinum toxin injections* for example, to smooth out crows’ feet, raise the eyebrows, act on the lion’s wrinkle, make eyes look larger, etc.
( *A film on botulinum toxin is available).
We should mention that these filling techniques using Botulinum toxin, or acting on the epidermis can also be carried out to postpone surgery by combating ageing symptoms from the outset or, with more limited results, on more marked patients who do not wish to undergo an operation.
THE OPERATION
Practical advice prior to the operation
Do not come morally or physically tired on the day of the operation. Let us know about any change in your state of physical or psychological health and do not forget that there is never any urgency to perform an aesthetic operation.
Medicines that cause bleeding are prohibited during the days preceding the operation: Aspirin, Anticoagulants, Vitamin E, etc.
It is imperative that all aesthetic operations be foregone if you are ill or, for women, if you are pregnant on the day of the operation. You must not drink or eat during the 6 hours prior to the operation. You must stop smoking due to the risk of necrosis. The operation will be cancelled if these recommendations are not heeded (fasting, no cigarette-smoking…).
When preparing your belongings, DO NOT FORGET YOUR MEDICAL FILE. Whenever possible, do not bring any valuable jewellery with you (or put it in the safe at the clinic with your other valuables during the operation.).
Take a shower or bath before coming to the clinic; wash your hair; women should obviously not wear nail varnish or make-up.
Where appropriate, arrange to have your hair permed or dyed prior to the operation (you will have to wait for one month after the operation before having your hair fixed again). Wear comfortable clothing when you come to the clinic.
It is imperative that contact lenses, dentures and hearing aids be removed before you are given an anaesthetic.
If you are also undergoing eyelid surgery and you are a contact lens wearer, you will not be able to use them for 5–10 days after the operation, so make sure you have a pair of glasses with you.
Anaesthesia and hospitalisation
Usually during these operations the patient is given a general anaesthetic and stays in the hospital for one to two nights.
For a simple Face Recurve® or facelift procedure involving a single area (e.g., neck or forehead alone), neuroleptanaesthesia (local assisted anaesthesia) can be administered on an outpatient basis. If this is the case, the patient usually leaves a few hours after the operation, unless it is preferable for them to stay in the hospital overnight due to post-op nausea or stress.
Leaving the clinic
Have clothes ready to wear that you do not have to put on over your head. If you want to leave the clinic incognito, bring a scarf, a hat or cap and sunglasses with you.
Operations requiring hospitalisation
Usually the patient can leave the hospital on the day after or two days after the operation.
Your hair will be shampooed before you leave the clinic. You will not have a bandage.
Outpatient procedures not requiring hospitalisation
Ask an ABLE-BODIED AND RESPONSIBLE person to take you home since anaesthetics are euphoriants. Furthermore, if you have undergone eyelid surgery, your vision could be blurred during the hours after the operation.
Do not make any plans to do anything that will require concentration or the use of potentially dangerous equipment. If you are going home by car YOU WILL NOT BE ABLE TO DRIVE UNDER ANY CIRCUMSTANCES.
Bring a pair of sunglasses with you if you want to leave the clinic more discreetly, but do not let go of the arm of the person accompanying you.
Before leaving home prior to the operation, make sure that you prepare everything for when you return:
– Prepare a light meal.
– Put Arnica 5CH, paracetamol-based painkillers (Dafalgan, Doliprane…), a bottle of mineral water.
Arrange for someone to be with you at home. You should not get up during the night following the operation without being accompanied even to go to the toilet and even if you feel perfectly fine (anaesthetics can cause effects identical to those of alcohol abuse).
The next stage
You should initially relax as much as possible and avoid any overexertion. However, you should walk a bit every day to prevent the risk of embolisms and eat enough to help with the healing process.
In the case of a neck or cheek lift, you may experience difficulties when eating due to discomfort when chewing. If this happens, it is the opportune moment to enjoy soufflés, chocolate mousses and other iced creams, but do not forget to brush your teeth as appropriate with a child’s tooth brush.
You will be able to wash your hair with a gentle shampoo from the next day on after the operation.
It is absolutely imperative that you do not smoke for 15 days after the operation in order to aid the healing process and reduce the risks of necrosis.
Note down the telephone number of the office (33 (0)1 45 53 27 17) and that of the clinic close to your home telephone and enter it into your mobile phone. Do not hesitate to call us if you are worried, for example if you have a temperature, oozing, pain or other symptoms that give you cause for concern.
Stitches are removed 15–20 days after the operation. If you have also undergone eyelid surgery, the eyelid stitches will be removed between 3 and 6 days after the operation.
Bruises usually persist for 10 to 20 days.
You can wear make-up from the 5 th day post-op. Do not hesitate to apply more masking products than you would under normal circumstances.
Swelling is at its height on the 3 rd to 4 th day after the operation then progressively fades. In addition to common methods such as the use of Arnica, cold compresses calm bruises and swelling and reduce their duration. It is also possible to help drain the face by temporarily adopting a sleeping position with the chest slightly raised.
Because of the tissue’s elasticity, skin re-draping will be performed with a slight hypercorrection, taking into account the secondary slackening of the skin. The skin will therefore look overly taut for a few weeks.
Summing it up, it will most probably take:
– seven days before being presentable enough for those close to you to see you and for you to be able to go out in public without being stared at;
– twelve to fifteen days before meeting up with friends… and going back to work;
– but it will be necessary to wait for 3 weeks to 1 month before meeting up with people close to you whom you do not want to know about the operation.
Caution: The consequences differ a lot depending on the reactions of each individual AND the degree of sophistication of the operation performed.
– For example, the postoperative period for a combined Face Recurve® Lift and concentric malar facelift procedure is more eventful than for a conventional facelift / eyelid procedure owing to the added localized treatments associated with Face Recurve®. A leave from work is therefore planned to last 10 to 15 days for a standard facelift versus 15 days to 3 weeks for a combined cervico-facial Face Recurve® and Concentric Malar Lift procedure, preferably.
– The swelling is a specific individual-related reaction which can also be influenced, however, by external factors such as food intake, the sleeping position, and the room temperature. For instance, it has been proven that it is better to lie sleeping with the head slightly raised to help evacuate the oedema; that an excessively warm bedroom promotes swelling and that an adequate diet, provided it be strictly followed and medically acceptable, will significantly reduce oedema.
Furthermore, bruises, swelling and possible hardening always vary on both sides of the face, so that temporary asymmetry after the operation is almost the rule, but this has no bearing whatsoever with the final outcome.
When planning on an operation, give yourself some time and take your obligations into account. Remember that even though the luckiest can show themselves to the world sooner than expected, it may happen – although this has no bearing on the end result, that you have to put up with an “interminable” recovery period and that you have to show just how patient a patient can be!
Shortcomings and specific operation-related specific risks
In most cases, the operations go smoothly and the patients are satisfied. Still, before you make your decision you should know the risks of possible shortcomings and complications.
General risks related to all surgery: infections, haematomas, healing problems and risks due to anaesthetics
Infections
If an operation is performed under normal conditions and post-op care and advice are adhered to, infections are very seldom. Namely, you will be asked to wash your hair daily at the beginning to keep the scars clean and to conform to the antiseptic and antibiotic prescriptions.
Haematomas
This complication, which requires rapid evacuation, is the problem most commonly encountered. It occurs during the hours immediately after the operation, which is why dressings are limited to scars and the face is not bandaged up as a rule so that it is possible to observe the face and notice any problem that should occur.
The risk of haematomas rises considerably when medicines that can cause bleeding are taken pre and post -op. Haematomas have also been reported when airplane travel is made too soon after surgery, and are brought on by the changes in atmospheric pressure.
Healing problems
Immediately after surgery, the scar may become inflamed or ooze; this requires specific, local, and often protracted treatment. Heeding to the advice concerning cleanliness, smoking cessation and the attendance of follow-up appointments is a decisive factor.
At mid-term follow up, the scar can sometimes develop unfavourably: thickening, widening, keloid formation. The same depends primarily on the type of skin (there are more problems with red-haired or black skinned individuals) and on the lifestyle (cigarette-smoking and contraceptive pills increase this risk).
Anaesthesia -related risks
Anaesthetic techniques and monitoring methods have improved immensely and safety is high when an operation is performed under non-emergency conditions on a person in good health, and when the anaesthetist is competent and practicing in a recognised establishment. However, anaesthetics can have unpredictable effects on the body, which can be potentially difficult to treat. Therefore, risks and hazards are still inherent to all anaesthesia before and after the operation. This is why it is imperative that you consult the anaesthetist prior to the operation and give him/her a detailed account of the state of your health. In accordance with your health and the planned operation, he/she will assess the anaesthetic risks and tell you of any potential precautions to take. If the anaesthetist objects to the operation, his/her decision is final.
(see in chapter ” Before surgery ” section “Check up and anaesthetic consultation“)
Risks during any aesthetic operation: asymmetries, results judged as insufficient or excessive, and the possible need for touch up corrections
Tissues always react specifically to surgery and, to some extent, unpredictably. This depends on the patient correctly following the doctor’s recommendations, but chance also plays a role. This is why all risks of asymmetry, unsatisfactory or excessive results and the need for touch up corrections are evoked prior to any aesthetic operation.
Procedure-specific risks
Partial facial paralysis
Thankfully, partial fa cial paralysis is extremely rare, but this risk must be mentioned. In most cases after-effects disappear naturally within the space of a few months, but in other cases it is necessary for the patient to undergo micro-surgery or to have Botulinum toxin injections to make the face symmetric, although it is not always possible to treat all of the consequences.
Skin necrosis
Skin necrosis is highly exceptional when recommendations regarding non-smoking are followed, yet this risk is high for inveterate smokers.
It should be known that the skin is usually irrigated by the network of veins both underneath and on the surface. During a facelift or a Face Recurve® Lift, the surgeon detaches and then stretches tissues that are re-draped towards the lateral edges of the face: ears, temples, forehead etc. Therefore, immediately after surgery, the skin is only supplied by the network of the superficial vessels. If, in addition, the micro-vessels are obstructed by tobacco (as in arteriosclerosis), the diameter of the superficial vessels becomes insufficient to ensure a good irrigation of the skin, particularly after the stretching through re-draping that further diminishes the vessels. Good tissue irrigation can be seen two hours after an operation in non-smokers, even for tissues furthest from the irrigation source (on the edge of the scars, in front of the ears). On the other hand, it may take too much time for the irrigation to return to the most remote zones when the patient is a smoker. The skin suffers and if the patient is unlucky, it dies for lack of irrigation; it becomes black at first before falling off. When this happens, it is necessary to wait for several months for granulation to take place, and then for new skin to grow, unless skin grafting is needed.
In addition to the risks involved, rejuvenation surgery also presents some disadvantages.
Such transient problems can affect the result and it is necessary to wait for longer than initially planned before benefiting from advantages of surgery. This is why a relationship based on trust between the patient and the surgeon is indispensable both before and after the operation.
Oedemas persisting in the malar area after more than three months.
These are systematically and completely absorbed but they always are difficult for patients to bear.
Transient scar retractions.
This problem proves particularly annoying when it occurs after rejuvenation surgery involving the mid-face of the concentric malar lift type. It is to be noted that all reoperation or trauma is to be utterly proscribed, as this would restart the inflammation process. There is only one solution: to wait.
Partial secondary tissue relaxing.
This problem affects men more frequently than women. It usually involves the neck and is related to the amount of skin removed and by too important a postoperative weight loss.
Hair loss in front of the scar.
When excess skin is removed by way of a scar running underneath the hair (primarily in the case of mask-lifts and vertical facelifts, much more rarely in the case of conventional facelifts and Face Recurve® Lifts), localized hair loss can arise, possibly requiring micro hair transplants.
Results
An initial evaluation of the final result can be made two to three months after the operation. However, scars and tissues may still be inflamed at that time. This is why, in order to assess the final result it is best to wait six to nine months after the operation.
Most often, an appreciable rejuvenation effect is achieved, giving a relaxed and refreshed appearance often coupled with a better psychological state.
As regards facelifts, the “baby skin effect” brought on by the healing process after the detachment of the skin is magnificent but always temporary. Unfortunately, it only lasts six to nine months. As mentioned in the introduction, facelifts are not particularly effective on the appearance of the epidermis; only skin abrasion techniques have long-term effects on the epidermis.
As far as rejuvenation surgery is concerned (facelift, Face Recurve® or Face Recurve® Lift), th e durability of the results depends greatly on health behaviour. The effects will be much more long-lasting if the patient refrains from sun exposure, important weight fluctuations and cigarette-smoking.
In the case of a age marker fascicle treatment, secondary ageing can also be improved on the areas not treated by a Concentric Malar Lift, Face Recurve® or Face Recurve® Lift, through Botulinum toxin injections in order to curtail further ageing due to face movements.
To conclude, we remind you that precise and detailed information, an in-depth analysis of the motivation for the operation, teamwork between the patient and the surgeon during the surgical program preparation phase, the search for surgical excellence coupled with a good analysis of benefits and risks, respect of pre-op and post-op recommendations, as well as regular monitoring of the patient are all key elements for aesthetic surgery to be a success.
References
Regarding Facelift surgery, some information is available in English in the pages « Facelift », « Midface lift » and « Forehead lift » of the ISAPS’website (International Society of Aesthetic plastic Surgery) section: « Info for patients ».
www.isaps.org
You can also find valuable information regarding the surgical rejuvenation in the pages « lifting cervico-facial » and « lifting fronto-temporal » of the SOFCPRE’s website (Société Française de Chirurgie Plastique Reconstructrice et Esthétique) : www.plasticiens.org
The spectacular progress of the sub-periostal face lift was initiated by Dr Paul TESSIER , see notably:
TESSIER P. : Le lifting facial sous-perioste – Subperiosteal face-lift
Ann Chir Plast Esthet. 1989;34(3):193-7.
http://www.ncbi.nlm.nih.gov/pubmed/2473674
Specific information delivered on this website is based on Doctor Le Louarn’s practice and on his scientific works:
1 – LE LOUARN C., BUTHIAU D, BUIS J. : Structural aging: the Facial Recurve concept
Aesthetic Plast Surg. 2007 May-Jun;31(3):213-8.
http://www.ncbi.nlm.nih.gov/pubmed/173803582 – LE LOUARN C., BUTHIAU D, BUIS J. : The Face Recurve concept: medical and surgical applications
Aesthetic Plast Surg. 2007 May-Jun;31(3):219-31; discussion 232.
http://www.ncbi.nlm.nih.gov/pubmed/174840583 – LE LOUARN C., BUTHIAU D, BUIS J. : Treatment of depressor anguli oris weakening with the face recurve concept
Aesthetic Surgery Journal, Volume 26, Issue 5, Pages 603-611C.
http://dx.doi.org/10.1016/j.asj.2006.08.0014 – LE LOUARN C., BUTHIAU D, BUIS J. : Rajeunissement facial et lifting malaire concentrique: le concept du FACE RECURVE®
Facial rejuvenation and concentric malar lift: the FACE RECURVE® concept
Ann Chir Plast Esthet. 2006 Apr;51(2):99-121.
http://dx.doi.org/10.1016/j.anplas.2005.12.016
http://www.ncbi.nlm.nih.gov/pubmed/165303165 – LE LOUARN C. : The Concentric Malar Lift and lower eyelid rejuvenation
Aesthetic Plast Surg. 2004 Nov-Dec; 28(6):359-72;
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&uid=156453386 – LE LOUARN C. : Chirurgie esthétique faciale par la voie d’abord palpébrale supérieure
Aesthetic facial surgery through the upper blepharoplasty incision JFORL vol 45/numero 4/1996
http://cat.inist.fr/?aModele=afficheN&cpsidt=32408627 – LE LOUARN C. : CORNETTE DE SAINT CYR B. : Incision Cutanée dans le Lifting Lambeau de SMAS Cervico-Malaire Oblique et Lifting Malaire
Cutaneous incision in facelift. Oblique cervicomalar SMAS flap and malar facelift.
Ann Chir Plast Esthet. 1994 Dec;39(6):756-64. French.
http://www.ncbi.nlm.nih.gov/pubmed/76615598 – LE LOUARN C. : The Malar S.M.A.S. flap
Elsevier – Plastic Surgery 1992 . Vol II. U.T. Hinderer, editor :517-18
http://cat.inist.fr/?aModele=afficheN&cpsidt=66800229 – LE LOUARN C. : Le Lambeau Musculo-Graisseux Malaire – The malar SMAS flap (The malar musculo-fatty flap)
Ann Chir Plast Esthet. 1989;34(6): 510-2, 1989
http://cat.inist.fr/?aModele=afficheN&cpsidt=6680022
http://www.ncbi.nlm.nih.gov/pubmed/2482693
Regarding Face lift surgery, the following publications and works can also be listed (this list is obviously not exhaustive and may be amended) :
1 – MENDELSON B.C., FREEMAN M.E., WU W., HUGGINS R.J. : Surgical anatomy of the lower face: the premasseter space, the jowl, and the labiomandibular fold
Aesthetic Plast Surg. 2008 Mar-Apr;32(2):185-95
http://www.ncbi.nlm.nih.gov/pubmed/181834552 – LITTLE J.W. : Structural aging: the facial recurve concept
Aesthetic Plast Surg. 2007 Nov-Dec ; 31(6):754-6.
http://www.ncbi.nlm.nih.gov/pubmed/179851773 – CORNETTE DE ST CYR B., GAREY L.J., MAILLARD G.F., AHARONI C. : The vertical midface lift. An improved procedure
J Plast Reconstr Aesthet Surg. 2007; 60(12):1277-86
http://www.ncbi.nlm.nih.gov/pubmed/175696064 – HAMRA S.T. : The role of the septal reset in creating a youthful eyelid-cheek complex in facial rejuvenation
Plast Reconstr Surg. 2004 Jun; 113(7):2124-41
http://www.ncbi.nlm.nih.gov/pubmed/152532085 – MENDELSON B.C.,MUAFFAR A.R., ADAMS W.P. Jr. : Surgical anatomy of the midcheek and malar mounds
Plast Reconstr Surg. 2002 Sep 1;110 (3):885-96
http://www.ncbi.nlm.nih.gov/pubmed/121721556 – BIGGS T.M. : Some thoughts on fixation in endoscopic brow lift
Plast Reconstr Surg. 2002 Jul ; 110(1):355-6.
http://www.ncbi.nlm.nih.gov/pubmed/120872937 – LITTLE J.W. : Three-dimensional rejuvenation of the midface: volumetric resculpture by malar imbrication
Plast Reconstr Surg. 2000 Jan;105(1):267-85; discussion 286-9.
http://www.ncbi.nlm.nih.gov/pubmed/106269998 – KNIZE D.M. : Muscles that act on glabellar skin: a closer look
Plast Reconstr Surg. 2000 Jan ; 105(1):350-61.
http://www.ncbi.nlm.nih.gov/pubmed/106270059 – ISSE N.G. : Endoscopic facial rejuvenation
Clin. Plast. Surg. 1997 Apr ; 24(2):213-31
http://www.ncbi.nlm.nih.gov/pubmed/914246610 – HAMRA S.T. : Composite rhytidectomy. Finesse and refinements in technique
Clin. Plast. Surg. 1997 Apr ; 24(2):337-46
http://www.ncbi.nlm.nih.gov/pubmed/914247211 – CONNELL B.F., MARTEN T.J. : The trifurcated SMAS flap: three-part segmentation of the conventional flap for improved results in the midface, cheek, and neck
Aesthetic Plast. Surg. 1995 Sep-Oct ; 19(5):415-20
http://www.ncbi.nlm.nih.gov/pubmed/852615712 – ISSE N.G. : Endoscopic facial rejuvenation: endoforehead, the functional lift. Case reports
Aesthetic Plast Surg. 1994 Winter ; 18 (1):21-913 – GOIN J.L. : Le lifting frontal, le lifting temporal, le «mask-lift» extra périosté
Frontal facelift, temporal facelift and extraperiosteal masklift
Ann Chir Plast Esthet. 1994 Oct;39(5):571-96
http://www.ncbi.nlm.nih.gov/pubmed/7771746
http://cat.inist.fr/?aModele=afficheN&cpsidt=425354514 – RAMIREZ O.M. : Aesthetic craniofacial surgery.
Clin Plast Surg. 1994 Oct ; 21(4):649-59.
http://www.ncbi.nlm.nih.gov/pubmed/781316315 – RAMIREZ O.M. : Endoscopic full facelift
Aesthetic Plast Surg. 1994 Fall ; 18(4):363-71
http://www.ncbi.nlm.nih.gov/pubmed/801721616 – RAMIREZ O.M. : Endoscopic techniques in facial rejuvenation: an overview
Aesthetic Plast Surg. 1994 Spring;18(2):141-7
http://www.ncbi.nlm.nih.gov/pubmed/801721617 – TREPSAT F., CORNETTE DE ST CYR B., DELMAR H., GOIN J.-L., THION A. : Les nouveaux liftings
39ème Congrès national de la SOF.CPRE (rapport annuel) sous la présidence du Dr F. VANDENBUSSHES
Ann Chir Plast Esthet. 1994 ; 39(5)18 – TREPSAT F., DELMAR H.: L’apport de la vidéo-endoscopie dans la chirurgie du rajeunissement de la face
Contribution of videoendoscopy to the surgery of face rejuvenation
Ann Chir Plast Esthet. 1994 Oct ; 39(5):647-65
http://www.ncbi.nlm.nih.gov/pubmed/777174919 – KAYE L.B. : Facelift surgery – Chapter 3 in Complications and Problems in Aesthetic Plastic Surgery
Edited by George C. PECK – Gower Medical Publishing 1992 : ISBN 0-397-44613-620 – KAYE L.B. : Forehead lift surgery – Chapter 4 in Complications and Problems in Aesthetic Plastic Surgery
Edited by George C. PECK – Gower Medical Publishing 1992 : ISBN 0-397-44613-621 – BIGGS T.M., KOPLIN L.: Concepts of neck lift – in Aesthetic Neck lift
Clinics in Plastic Surgery Vol 10 N°3 Jul 1983 : 367-78.- Edited by José Guerrerosantos – Saunders : ISSN 0094-1298
http://www.ncbi.nlm.nih.gov/pubmed/662783322 – GUERREROSANTOS J. : Neck lift. Simplified surgical technique, refinements, and clinical classification.
Clinics in Plastic Surgery Vol 10 N°3 Jul 1983 : 379-404 Saunders : ISSN 0094-1298
http://www.ncbi.nlm.nih.gov/pubmed/662783423 – REES T.D. : Aesthetic surgery of neck and face – Part 4 Volume II in Aesthetic Plastic Surgery
Edited by Thomas D. REES – Saunders 1980 : ISBN 0-7216-7521-2